
http://www.marksdailyapple.com/
 Contrary to what we’ve been told, cholesterol didn’t evolve to give us heart disease. It’s not here to kill us. The actual roles of cholesterol in the body include insulating neurons, building and maintaining cellular membranes, participating in the immune response, metabolizing fat soluble vitamins, synthesizing vitamin D, producing bile, and kick-starting the body’s synthesis of many hormones, including the sex hormones. Without cholesterol, it’s true that we wouldn’t have heart disease, but we also wouldn’t be alive.
Contrary to what we’ve been told, cholesterol didn’t evolve to give us heart disease. It’s not here to kill us. The actual roles of cholesterol in the body include insulating neurons, building and maintaining cellular membranes, participating in the immune response, metabolizing fat soluble vitamins, synthesizing vitamin D, producing bile, and kick-starting the body’s synthesis of many hormones, including the sex hormones. Without cholesterol, it’s true that we wouldn’t have heart disease, but we also wouldn’t be alive.
Given all the work cholesterol has to do, the liver is careful to ensure the body always has enough, producing some 1000-1400 milligrams of it each day. Dietary cholesterol is a relative drop in the bucket. And besides, the liver has sensitive feedback mechanisms that regulate cholesterol production in response to how much you get from your diet. Eat more cholesterol, make less in the liver. Eat less, make more in liver.
Now, if cholesterol is so important, why do we worry about it at all? How has it garnered such a bad reputation for giving us heart attacks?
History of Cholesterol and Heart Disease
Heart disease took off in the early part of the twentieth century, and doctors frantically searched for the cause throughout the next several decades. Early studies in rabbits found that feeding them dietary cholesterol reliably increased blood cholesterol levels and induced atherosclerosis that very much resembled human atherosclerosis. Human tests in the fifties initially showed an association between early death by heart disease and fat deposits and lesions along artery walls. Because cholesterol was found to be present in those deposits and because researchers had previously associated familial hypercholesterolemia (hereditary high blood cholesterol) with heart disease, they concluded that cholesterol must be the culprit.
And while it’s true that cholesterol is involved in heart disease, the direct cause-and-effect relationship has not been established. The reality is far more complicated. To get closer to the reality, we must first understand what these cholesterol numbers actually mean.
Cholesterol versus Lipoproteins
Back in those early rabbit studies, researchers discovered a curious thing: even though feeding the rabbits cholesterol spiked their blood cholesterol and gave them heart disease, bypassing the first step and injecting it directly into the blood had no effect. It was completely harmless.
As it turns out, cholesterol doesn’t normally float around the blood by itself. It is contained within lipoproteins. You can think of lipoproteins as delivery vessels. They contain cholesterol, antioxidants, and fatty acids and along the surface have various proteins that direct the lipoprotein to different sites around the body. It’s not the cholesterol that is involved with atherosclerosis. It’s the lipoprotein.
Let’s play the freeway analogy game. Both LDL-cholesterol (LDL-C) and HDL-cholesterol (HDL-C), the standard, basic readings you get from the lab, do not reflect the number of LDL or HDL lipoproteins, or particles, in your serum. Instead, they reflect the total amount of cholesterol contained in your LDL and HDL particles. Hence, the “C” in LDL/HDL-C, which stands for “cholesterol.” Measuring the LDL/HDL-C and then making potentially life-changing health decisions based on the number is like counting the number of people riding in vehicles on a freeway to determine the severity of traffic. It’s data, and it might give you a rough approximation of the situation, but it’s not as useful as actually counting the number of vehicles. A reading of 100 could mean you’re dealing with a hundred compact cars, each carrying a single driver, or it could mean you’ve got four buses carrying 25 passengers each. Or it could be a couple buses and the rest cars. You simply don’t know how bad (or good) traffic is until you get a direct measurement of LDL and HDL particle number.
How does this relate to heart disease?
In my opinion, the most convincing heart disease hypothesis goes like this:
- LDL receptors normally “receive” LDL particles and remove them from circulation so that they can deliver nutrients and cholesterol to cells, and fulfill their normal roles in the body.
- If LDL receptor activity is downregulated, LDL particles clear more slowly from and spend more time in the blood. Particles accumulate.
- When LDL particles hang out in the blood for longer stretches of time, their fragile polyunsaturated fatty membranes are exposed to more oxidative forces, like inflammation, and their limited store of protective antioxidants can deplete.
- When this happens, the LDL particles oxidize.
- Once oxidized, LDL particles are taken up by the endothelium – a layer of cells that lines the inside of blood vessels – to form atherosclerotic plaque so they don’t damage the blood vessel. This sounds bad (and is), but it’s preferable to acutely damaging the blood vessels right away.
- So it’s the oxidized LDL that gets taken up into the endothelium and precipitates the formation of atherosclerotic plaque, rather than regular LDL. OxLDL, poor receptor activity, and inflammation are the problems.
If that’s the case, what exactly is the deal with traditional blood lipid numbers—the ones you get on a standard blood test?
This information is how I view cholesterol as it relates to my individual biology. If you have questions about your cholesterol numbers, discuss them with a qualified health professional.
Total Cholesterol
Standard view: Get that TC below 200, or else you’ll have a heart attack or you’ll have to pay a higher health insurance premium, if the insurers take you on at all.
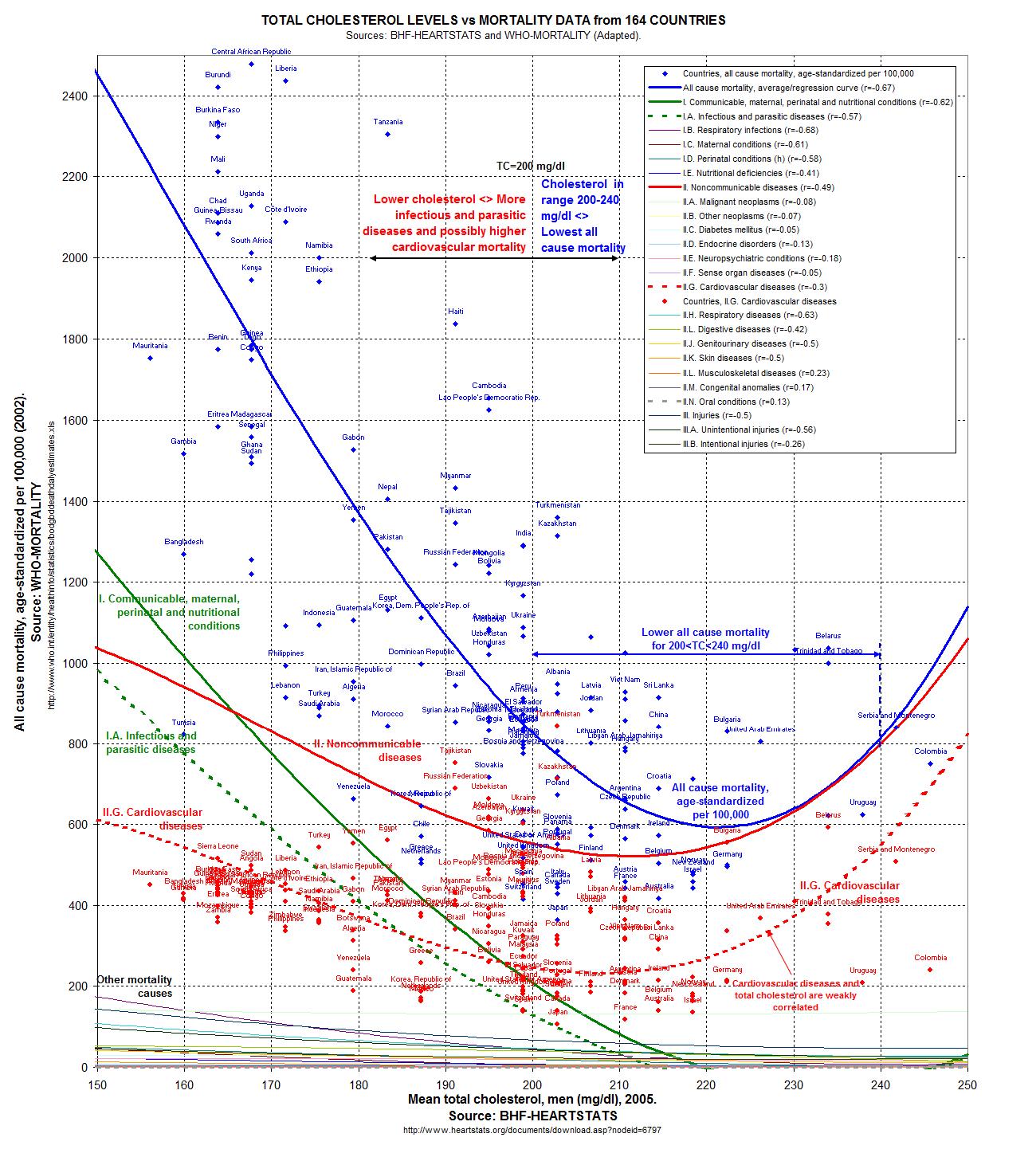
My take: Mostly meaningless. Even though the epidemiological evidence suggests a TC between 200 and 240 mg/dl is best for all-cause mortality,1 we can’t hang our hats on it. First off, total cholesterol is limited because it’s only telling us the amount of cholesterol contained in all our lipoproteins without saying anything about what kind of lipoproteins we have or how many there are. Second, total cholesterol is limited because it’s determined by a bizarre formula – HDL-C+LDL-C+(Triglycerides/5) – that reduces various types of blood lipids, each with a different role in the body and a unique impact on our risk for illness, to mere numbers. Someone with low HDL and high triglycerides could easily have the same TC as someone with high HDL and low triglycerides, so long as the numbers work out. Whether it’s being used to predict wellness or disease, total cholesterol by itself is mostly meaningless.
HDL Cholesterol
Standard view: “Good” cholesterol. It’s the “garbage truck” that cleans up “excessive” cholesterol and fat from tissues, so the higher the better! Though men and women should strive for levels exceeding 60 mg/dl, above 40 is acceptable for the former and above 50 is acceptable for the latter.
My take: Higher HDL-Cs correlate strongly with better cardiovascular health. No real argument here. Higher HDLs are desirable. Just remember, it’s only a snapshot of a glimpse into the cholesterol content of your HDL particles. Among most groups tested, the TC:HDL ratio is actually a strong indicator of heart disease risk, with higher ratios corresponding to higher risks. Note, though, that no Primal Blueprint adherents were among the groups analyzed, ever.
LDL Cholesterol
Standard view: Get it as low as humanly possible! I want that low density lipoprotein so low as to be nearly nonexistent. Your body obviously hates you; otherwise, it wouldn’t be producing a potently toxic substance and sending it directly into your endothelial cells to form atherosclerotic plaque! Of course, we’re not actually measuring the number of low density lipoproteins, just the amount of cholesterol contained in them, but still!
My take: While a high LDL-C may indicate a problem, remember that LDL-C only indicates the total amount of cholesterol in your LDL particles. You could easily have a few large particles (good) or a bunch of smaller, denser ones (bad, might indicate poor LDL receptor activity and an LDL that likes to hang out in the blood), but LDL-C alone isn’t enough to know. It’s also just a moment in time, whereas what you’re interested in is the trend. If the trend indicates a steady rise in LDL-C, however, that could hint at poorer LDL clearance and lower LDL receptor activity (and greater susceptibility to oxidation).
Triglycerides
Standard view: Lower would be better, sure, but you really gotta do something about that LDL! Anything less than 150 mg/dl is fine.
My take: High triglycerides correlate strongly with low HDL and smaller, denser LDL. High triglycerides, then, could indicate more oxidized (or oxidizable) LDL. The triglycerides of most Primal eaters, especially those on the lower carb side of things, usually hover well below 100 mg/dl. Triglycerides come packaged in VLDL, or very low density lipoproteins (which are calculated by dividing your triglyceride count by 5).
So, what can we learn from a standard lipid test? If we take a series of regular ol’ lipid measurements, preferably one pre- and several peri-Primal, we can get an idea of our metabolic health. Look for:
- Trends – Are your triglycerides going down over time? That’s great. Is your HDL trending up? Also good.
- Normal fluctuations – Your numbers can jump around 20-30 points in either direction between readings without it necessarily meaning anything.
- TC:HDL-C ratio – Lower is better and indicates fewer LDL particles.2
- Triglyceride:HDL-C ratio – Lower is better and indicates larger LDL (and, usually, fewer) particles. Ideally, this will be close to 1 or lower; one study (PDF) found that 1.33 was the cut off.34
There is an advanced lipid test that’s worth getting: ApoB.
Apolipoprotein B
Every single LDL particle has a single ApoB, making ApoB an effective measurement of LDL particle count. By all accounts I could find, ApoB is reliable and accurate. Every LDL particle has one ApoB, and along with TC:HD ratio, ApoB count is a strong predictor of heart disease risk (again, with the caveat that these studies are on populations leading a decidedly unPrimal and highly inflammatory lifestyle).5 If you have a lot of ApoB, you have a lot of LDL particles, which could mean the LDL receptor activity is down-regulated. Or, it could mean you’re losing weight, which can affect lipid values in multiple ways. Or, it could mean that today was a particularly “high ApoB day” and that getting it tested next week will give a different result, simply due to natural fluctuations. You just don’t know.
And that’s actually the main issue with all cholesterol readings, however advanced: They are snapshots in time. They do not capture the natural fluctuations and trends of the biomarkers. Your cholesterol was elevated today at 12 noon. What does that say about your levels tomorrow at six in the evening? Next week? Nothing. To account for natural fluctuations, get tested at regular intervals and observe the trends.
If you can’t get the ApoB test, total cholesterol/HDL ratio is a good indicator of how long LDL is hanging around in the blood and remains the best standard assessment of heart disease risk. Another good one is triglyceride/HDL ratio, which is a strong surrogate marker for insulin resistance. In both cases, lower is better. An ideal T/HDL ratio is 1:1; 2:1 is about as high as you want to go. An ideal TC/HDL ratio is 3.5:1 or lower.
Okay, so by whatever metric you want to use, your numbers are “elevated” and you’ve taken enough readers to get a general trend. It’s not just an isolated number. Should you worry?
Is High Cholesterol a Problem?
Oh, boy. There’s the million dollar question.
First off, let’s go back to the evolutionary prism. As a naturally self-regulating system, the body isn’t going to produce something that is intrinsically pathological. Maybe that could happen in really rare genetic mutations, but everyone produces, utilizes, and relies upon cholesterol. It simply doesn’t make sense that cholesterol is evil.
Adequate cholesterol isn’t available for the body’s repair system, for the uptake of serotonin, for the full initiation of Vitamin D and hormone production and their regulation of blood sugar and inflammation, etc., etc. What does your logic tell you here? Yup, nothing is running the way it should.
Let me also add that everyone’s cholesterol profile is going to be different, no matter what. And I acknowledge that a very small percentage of people out there genuinely have *true* hereditary high blood cholesterol, familial hypercholesterolemia, a metabolic condition with impaired or even lack of ability to metabolize cholesterol. This condition can have serious health consequences. By the way, this condition, in its heterozygous form affects at most 1 in 500 people. Total serum cholesterol in these folks is in the 400 mg/dl range (as opposed to the 200 recommended). The homozygous form affects about 1 in 250,000. You likely don’t know anyone in this category because their disorder almost always ends their lives at a very young age. But even the heart disease common in familial hypercholesterolemia might not be caused solely by high LDL, but by poor coagulation.6
But if you’re eating a healthy diet, your performance is good, your body comp is good (or trending that way), your energy and sleep are rock-solid, you don’t have any familial hypercholesterolemia genes—is it really dangerous to have elevated cholesterol numbers?
I don’t know. But I’m skeptical.
For one, “elevated” cholesterol isn’t necessarily linked to heart disease. Sometimes it’s even linked to lower mortality. For instance, in people older than 60, high LDL is associated with lower all-cause and cardiovascular mortality.7 That’s right: higher LDL, less heart disease deaths. Plus, most people who have major heart attacks have “normal cholesterol.”
I’ve said it before, and I’ll say it again. Sound and reliable medical research hasn’t proven that lowering (or low) cholesterol in and of itself reduces risk of death from heart disease across a population. What does this tell you? There must be some other piece or pieces to the cholesterol/heart disease story.
Based on my examination of the evidence over the years, it all boils down to oxidative stress and inflammation.
The inflammatory response and subsequent oxidative stress load is ultimately responsible for the oxidation of the LDL, while inflammatory cytokines produced at the atherosclerotic site can weaken and loosen the plaque, thus setting the stage for (and even causing) a rupture. In fact, inflammation is intimately involved in nearly every aspect of heart disease.89
Furthermore, nearly every study suggests that LDL is only a true threat when it’s oxidized. What increases the risk of oxidized LDL?
- Having LDL particles that hang out longer in the blood.
- Eating too much linoleic acid (it’s the polyunsaturated fat in the lipoprotein that oxidizes).10
- Being deficient in vitamin E.
- Having type 2 diabetes and/or high blood sugar.11
- Failing to eat grass-fed dairy.12
- Not exercising.13
- Not eating extra virgin olive oil and fish oil.14
To name a few. Could “high” LDL particles be closer to benign if they’re more resistant to oxidation? I would imagine so. Does resistance mean immunity to oxidation? Absolutely not. Don’t get cocky.
Substantially “elevated” cholesterol, low HDL or high LDL can be a real problem, but they may also just be a symptom of the larger concern rather than the main issue itself. Cholesterol profile can be impacted by other conditions such as hypothyroidism, untreated diabetes or pre-diabetes, pregnancy (surprise!), lactation, stress, liver conditions, heart disease (symptom, not cause of). Even weight loss or fasting can spike cholesterol numbers (turns out burning all that animal fat off your body can have a momentary effect on blood lipids). Talk to your doctor about what your numbers mean in the grand scheme of your health. And see if you can get a read on other markers, like C-reactive protein (an inflammatory indicator), oxidized LDL, and ApoB (or some other marker of LDL particle number).
High cholesterol shouldn’t be ignored, but it’s not the only thing that matters. You have to look at the whole picture. You have to take a step back (or several steps back) and consider everything—not just numbers on a readout.
If you have any more questions about this topic, drop them down below. Thanks for reading, everyone. Take care.
References
- http://perfecthealthdiet.com/wp/wp-content/uploads/2011/06/O-Primitivo-Cholesterol.jpg
- https://www.ncbi.nlm.nih.gov/pubmed/19903920
- https://www.ncbi.nlm.nih.gov/pubmed/19091534
- https://www.google.com/url?sa=t&rct=j&q=hdl%20tg%20ratio&source=web&cd=4&ved=0CE8QFjAD&url=http%3A%2F%2Fcare.diabetesjournals.org%2Fcontent%2F23%2F11%2F1679.full.pdf&ei=mvPxTrDtMY7XiALm8OW5Dg&usg=AFQjCNE3GzGevscRzugAZXArj9BWCqn9eA&sig2=nhtWZ_ze7r3xudNliKrTYQ
- https://www.ncbi.nlm.nih.gov/pubmed/19903920
- https://www.sciencedirect.com/science/article/abs/pii/S0306987718304729
- https://pubmed.ncbi.nlm.nih.gov/27292972/
- http://atvb.ahajournals.org/content/20/6/1536.full
- https://www.ncbi.nlm.nih.gov/pubmed/16470012
- https://www.sciencedirect.com/science/article/abs/pii/0891584993900745
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4940560/
- https://pubmed.ncbi.nlm.nih.gov/21591986/
- https://pubmed.ncbi.nlm.nih.gov/29190851/
- https://pubmed.ncbi.nlm.nih.gov/10451477/
The post The Definitive Guide to Cholesterol appeared first on Mark’s Daily Apple.
Filed under: Fitness
 For now classes are 6pm and 640pm at 2840 Wildwood st in the Boise Cloggers studio.
Book your class NOW!
click this ==>
For now classes are 6pm and 640pm at 2840 Wildwood st in the Boise Cloggers studio.
Book your class NOW!
click this ==>








{kind=link}