Ugh. The other day I walked away from a pot of sautéing onions for all of two minutes (okay, maybe more like 10 minutes), and came back to find this blackened, burned-on mess. Not only was my soup recipe ruined, I worried that my enameled pan was, too.
Happily, the method I’ll show you here not only saved my pot, it kept me from having to soak it for hours, or worse, risk ruining the enamel with an abrasive scrub. All that’s needed is one secret weapon I already had in my kitchen.
pimg class=”alignright size-full wp-image-55008″ src=”http://cdn.marksdailyapple.com/wordpress/wp-content/uploads/2015/04/Orange-Chicken4.jpg” alt=”Primal orange chicken” width=”320″ height=”212″ /Orange chicken probably needs no introduction, but for those of you who have never ordered from a Chinese-American take-out menu, it’s battered and deep-fried chicken pieces coated in a sticky, sweet orange sauce. Health food, it is not. But sometimes, it’s surprisingly easy to transform a recipe from something a title=”Eliminate SAD Foods” href=”http://www.marksdailyapple.com/action-item-1-eliminate-sad-foods/#axzz3WZPC7xVk%20″SAD/a into something deliciously Primal./p
pThis Primal Chinese Orange Chicken recipe takes what’s good about Orange Chicken (crispy morsels of chicken and a sweet, tart, spicy sauce) and leaves out what’s bad (flour, cornstarch, canola oil, sugar). The orange sauce – made mainly from freshly squeezed orange juice, a title=”Are Coconut Aminos Primal? ” href=”http://www.marksdailyapple.com/is-it-primal-7-more-foods-scrutinized/#axzz3WkF476BN”coconut aminos/a and rice vinegar #8211; is so good that it makes a person wonder why sugar is ever added in the first place. And the bits of chicken #8211; tender in the middle […]
div class=”breakout”
pIt’s Friday, everyone! And that means another a title=”Success Stories” href=”http://www.marksdailyapple.com/category/success-story-summaries/” Primal Blueprint Real Life Story/a from a Mark#8217;s Daily Apple reader. If you have your own success story and would like to share it with me and the Mark’s Daily Apple community please contact me a title=”Contact Me!” href=”http://www.marksdailyapple.com/the-book/share-success-story/” target=”_self”here/a. I’ll continue to publish these each Friday as long as they keep coming in. Thank you for reading!/p
/div
pimg class=”alignright” src=”http://cdn.marksdailyapple.com/wordpress/wp-content/uploads/2014/10/real_life_stories_stories-1-22.jpg” alt=”real_life_stories_stories-1-2″ width=”320″ height=”240″ /I remember my senior year of high school before deciding to go Primal. I went to a small high school just outside of Milwaukee, Wisconsin, and was a two time state qualifier in track in field for the 4#215;200 meter relay. I ran sprints in track in the spring, and ran cross country in fall to stay in shape and work on running form. As you can guess with all this constant working out (especially […]
pimg class=”alignright size-full wp-image-54996″ src=”http://cdn.marksdailyapple.com/wordpress/wp-content/uploads/2015/04/play.jpg” alt=”boy climbing on wall” width=”320″ height=”213″ /I always find it funny when I write about something and suddenly I find other incredible angles of the topic coincidentally pop up in my newsfeed or even conversation. (I also loved reading the gamut of stories and opinions on the board.) Such was the case a couple weeks following my post on a title=”Are We Thwarting Our Children’s Instinct to Explore?” href=”http://www.marksdailyapple.com/are-we-thwarting-childrens-instinct-to-explore/”free-range kids/a. It’s true some other major media outlets took up the general subject in their op-eds, etc. More interestingly, I’ve stumbled across commentaries that cover everything from the a title=”Why Tree Climbing is Good for Children” href=”http://www.telegraph.co.uk/lifestyle/wellbeing/outdoors/11512054/Why-tree-climbing-is-good-for-children.html” target=”_blank”value of tree-climbing/a to the a title=”What Would My Mom Do: Drink Tab and Lock Us Outside” href=”http://community.today.com/parentingteam/post/what-would-my-mom-do-drink-tab-and-lock-us-outside” target=”_blank”no-fuss, no-guilt philosophy/a of 70s mothers (as the title notes, drinking Tab and locking us outside). Sound familiar to anyone?/p
pspan id=”more-54994″/span/p
pThe […]
What conditions is low-dose naltrexone effective for? There are actually two ways to answer this question. The first is what the scientific literature shows, and then the second is what clinical and anecdotal experience of clinicians that are working with LDN shows.
In this episode, we cover:
3:36How LDN works 10:50 The effectiveness of LDN 17:25 Finding a doctor to work with
[powerpress]
Steve Wright: Good morning, good afternoon, and good evening. You are listening to the Revolution Health Radio Show. I’m your host, Steve Wright, co-author at SCDlifestyle.com. This episode of the RHR podcast is brought to you by 14Four.me. This is a 14-day healthy lifestyle reset program. Chris has put together a really simple, step-by-step, hand-holding program for those of you who are still struggling with sleep issues, weight issues, gut issues — actually basically any health issues — because the 14Four.me program addresses your food, your sleep, your movement, and your stress, all foundational principles for living a long, healthy life and overcoming any sort of chronic conditions you’re still dealing with. If you’re having problems implementing these in your life, please check out 14Four.me. It might be the program for you.
With me is integrative medical practitioner, healthy skeptic, and New York Times bestselling author, Chris Kresser. Chris, how are you doing?
Chris Kresser: Pretty well. How are you, Steve?
Steve Wright: I’m catching up on some sleep, but I’m doing well.
Chris Kresser: All right. Yeah, I heard you’ve been out partying hard at Garth Brooks concerts!
Steve Wright: I can’t say I haven’t been. It’s been good to put on the Stetson, the cowboy boots, and sing some Friends in Low Places.
Chris Kresser: That’s pretty awesome. I have to remember you’re Midwest born and raised, right?
Steve Wright: Yeah, yeah, coming from the rural backwoods of Michigan. Not really that backwoods, but —
Chris Kresser: That’s great.
Steve Wright: — I got the country gene.
Chris Kresser: Good times, good times.
Steve Wright: Yes.
Chris Kresser: All right, so we have a great question this week. It was actually hard for me to believe that I had never covered it. I’ve talked about it on so many different podcasts and in blog articles and stuff, but I realized when we got this question that I had never actually covered this topic in one distinct podcast, so here we go.
Question from Larry: Hi, Chris. My name is Larry Leibowitz. I’m an integrative/functional family physician in Connecticut. I’ve become an avid listener to your podcast, and I find a lot of the material to be extremely useful and very helpful for my practice. As you can imagine, I see a lot of patients with chronic inflammatory conditions. Many of them are autoimmune in nature, and recently I’ve been considering the use of low-dose naltrexone with my patients. I’d be very interested in hearing about your experiences with the medication, some of the successes and/or failures, and in which cases you find it to be the most useful. Thanks. Take care.
Chris Kresser: All right. Yeah, like I said, it’s something we’ve talked about here and there, and it can be really useful for people with autoimmune conditions. I think a lot of folks have heard of it by now, but I want to just take the chance to give a little bit of background, explain how LDN, low-dose naltrexone, works, what kind of conditions it’s been studied in and might be effective for, and we’ll talk about some pros and cons and things to keep in mind if you take it and how you might find a doctor that you can work with to take it.
How LDN works
As the name implies, low-dose naltrexone is a low dose of a medication called naltrexone that was originally approved back in the ’80s at a higher dose, 50 mg, for the purpose of helping opiate and heroin addicts to get off those drugs, and it works by blocking the reception of opioid hormones. So if you were on a 50 mg dose, you could take any kind of opiate drug and not get high. But the problem was that in addition to not getting high when taking these opiates, people who were taking 50 mg of naltrexone didn’t feel any pleasure at all because the opioid receptors in our brain mediate our experience of pleasure. So at the full dose, naltrexone really reduced that experience of pleasure and, therefore, wasn’t a very sustainable or effective drug.
But around that time in the mid ’80s there was a doctor in New York named Dr. Bihari who was interested in treating cancer and AIDS, which was just becoming something that people were starting to focus on more at that point, of course, and he discovered that a low dose between 3 mg and 4.5 mg of naltrexone had beneficial effects on the immune system. And since then, LDN has been used for autoimmune disease, cancer, and other conditions that involve immune dysregulation. This is important to understand if you’re going to talk to your doctor about LDN because a lot of doctors might be familiar with naltrexone that was used for this purpose and might raise their eyebrows or not be familiar with the fact that a lower dose is used for a completely different purpose. The higher dose is about blocking opioid receptors and detox and getting people off drugs, whereas the low dose is being used now for balancing and regulating the immune system, so it’s important to make that distinction.
Without getting too geeky here, I want to tell you a little bit about how LDN works because it’s interesting, and it, of course, helps to understand how it might benefit you if you have an immune-related condition. And this is ongoing. There are new papers published about the mechanisms of LDN each year, and we’re still learning about this, but so far, there are two main mechanisms that have been identified. One is that, as I said, it regulates the immune system, and it does this primarily by promoting T regulatory cell function. The T regulatory cells, or Tregs, they keep the immune system in balance, and they turn inflammation on and off, depending on what’s needed, and they prevent the immune system from getting stuck in patients with overactive immune systems, like people with allergies or asthma or autoimmune conditions. The way this works is LDN, as I mentioned, it temporarily blockades the opioid receptors in the brain, and when the receptors are blocked, the body thinks more opioids are needed, and so it produces more, and by the time more opioids are produced, LDN is out of the system, the receptors are unblocked and receive those, and that leads to essentially a net increase in opioid production.
So if you’re wondering now, like, what does this have to do with the immune system, we now know that people with autoimmune disease often have low levels of these opioids and that white blood cells, which, of course, are what are driving the immune response, have receptors for these opioids, which, of course, suggests that they play a really important role in the immune system.
So that’s number one, this immune-regulating, balancing mechanism.
Steve Wright: Does the increase in opioids actually then cause a corresponding increase in Treg cells? Is that the point you were making there?
Chris Kresser: Yeah, exactly. And then the Treg cells are the ones that — I mean, they’ve been referred to as the police force of the immune system. I’m not sure that’s the best analogy these days, given what’s been happening, but the idea is that they balance and regulate the immune system and keep both sides in check.
Another more recently discovered mechanism is that LDN reduces inflammation in the central nervous system, and the significance of this is that inflammation in the central nervous system is thought to play a role in a number of different conditions that LDN has been shown to be effective for, like fibromyalgia and chronic pain and depression. In addition to blocking the opioid receptors, LDN blocks something called toll-like receptor 4 that’s found on white blood cells that are called microglia, and the microglia are central nervous system immune cells that produce inflammation, pain sensitivity, fatigue, sleeplessness, mood disorders, and cognitive problems. When those microglia are chronically activated, as they are fibromyalgia and other pain disorders, it results in neurotoxicity and then this whole wide cascade of symptoms that are associated with all these conditions, and LDN essentially blocks that cascade by blocking the receptors on those microglial cells. This probably explains why in some of the studies so far LDN has been shown to reduce something called erythrocyte sedimentation rate, or ESR, which is an inflammatory marker that’s elevated in conditions like fibromyalgia.
Again, to recap, there are two basic mechanisms: balancing and regulating the immune system and then reducing central nervous system inflammation. There probably are other mechanisms, but those are the ones that have been the most clearly defined so far.
Steve Wright: Chris, is there any way for people to test their opiate levels to know if they might be low and LDN would be an ideal —
Chris Kresser: Not that I’m aware of. There are some tests that can look at various kinds of immune cells and the balance between those immune cells, but they’re not widely available and they’re a little bit difficult to interpret, so it’s not something that I think is that useful for the average person or ready for primetime. I think with LDN the best way to determine if you’ll benefit from it is whether you have the conditions that it’s shown to be useful for or any other kind of immune-related condition and then just doing a therapeutic trial, but we’ll talk a little bit more about that in a second.
The effectiveness of LDN
OK, so what conditions is LDN effective for? There are actually two ways to answer this question. The first is what the scientific literature shows, and then the second is what clinical and anecdotal experience of clinicians that are working with LDN shows. There’s definitely research out there on LDN, but it’s still somewhat limited, and I think clinical and anecdotal experience is further ahead in terms of the breadth of conditions that LDN is being used for and the experience of how effective it can be for those conditions. The studies are also still usually relatively small sample size, not always randomized, not always double-blinded. Part of the reason for this is they’re probably not that well-funded because low-dose naltrexone is off patent, and that means that drug companies don’t stand to make a killing on selling LDN, and it’s unlikely that a whole lot of money is going to be put into it for that reason.
Having said that, the results so far of the studies on LDN have been really encouraging, and they’ve been primarily on cancer, multiple sclerosis, Crohn’s disease, fibromyalgia, and autism. It’s especially effective for Crohn’s with over a 70% remission rate and even complete mucosal healing as evidenced by colonoscopy in some cases. If you know about Crohn’s disease and how nasty it can be and how difficult to treat and how poor the success rates are of the typical treatments, that’s a pretty remarkable statistic, over 70% remission rate with mucosal healing, especially when you consider the fact that there were not documented side effects of LDN in that study compared to placebo.
So that’s what’s in the scientific literature, but anecdotally clinicians are using it for a whole wide range of conditions involving inflammation and immune dysregulation, autoimmune diseases like Hashimoto’s and Graves’, rheumatoid arthritis, lupus, psoriasis, chronic fatigue syndrome, neurodegenerative disorders like Parkinson’s and Alzheimer’s. It’s being extensively used for infertility. There’s a clinic in the United Kingdom that is basically almost entirely focused on using LDN for fertility to treat patients who are struggling with that. And the reason it’s effective for such a broad range of conditions is because of the mechanism of action. As I said, it regulates and balances the immune system and reduces inflammation, and of course, we know that inflammation and immune dysregulation are at the root of many diseases and certainly at the root of autoimmune conditions. Even though there aren’t any studies of LDN on Hashimoto’s, for example, it makes sense that it would work for Hashimoto’s if it’s working for multiple sclerosis and Crohn’s disease because the underlying mechanism of all those conditions is immune dysregulation, autoimmunity. That’s why a lot of clinicians out there feel justified and safe in using LDN for conditions that it hasn’t directly been studied on because, A, the mechanism makes sense and, B, it’s safe and well tolerated and doesn’t have any significant complications or risks or even side effects in many of these studies.
One of the advantages of LDN as a therapy is that it’s low cost. It’s off patent, as I said, which means typically you can get it for about 40 bucks a month, 35 or 40 bucks a month from a compounding pharmacy.
The side effects are pretty minimal, in that in some of the double-blind, placebo-controlled trials, as I said, there was no difference in side effect between placebo and the treatment group, but I will say that in our experience, what we’ve seen in our clinic and other clinicians I know that work with it, there are some side effects that are fairly common, which are temporary sleep disturbance when a patient first starts taking it or vivid dreams and a mild headache, but these usually pass pretty quickly and can often be mitigated by starting with a lower dose, so if 3 mg or 4.5 mg is the ultimate dose that they end up on, starting at, like, 1 mg or 1.25 mg or something and then building up more slowly.
LDN does not have any known abuse potential. It’s not an addictive medication. One of my hesitations or criticisms of a lot of drugs is that they just primarily work by suppressing symptoms and they don’t necessarily improve the function of the body, but LDN is a little different in that respect, in that it works by improving the function, it increases the production of T regulatory cells, which then have that immune-balancing effect and, I think, makes it a little bit safer to use over the long term. Now, of course, if you can achieve results and address your autoimmune condition without using a medication, even one as safe as LDN, then that’s great, but my rubric for a treatment, you know, whether a treatment makes sense, has always been whatever is the most effective and causes the least amount of harm. In many cases, that’s not a drug, but LDN is actually one medication that I think passes that test.
One of the disadvantages of LDN is that there’s still not standardized dose, and really the patient and the prescribing physician just kind of have to figure it out through trial and error. From our experience, we’ve seen most people end up around 2.5 mg to 3 mg; 4.5 mg tends to be too much for people. I’ve seen some patients settle on as little as 1.25 mg or 1.5 mg, but anywhere in the 1 mg or 1.25 mg to 4.5 mg range could be the optimal dose for a given person.
We still need more research. I mentioned that the research we have already is somewhat limited, so we need more research.
Finding a doctor to work with
It’s not always easy to get a prescription. A lot of primary care doctors aren’t familiar with it. It’s not covered by insurance. It’s completely off label, but fortunately it’s pretty cheap. Even if people are paying out of pocket, it’s only about 35 or 40 bucks a month.
And although all the studies we have so far show that it’s safe, we don’t have any hard data on really long-term safety, you know, people who have been taking LDN for 10 years or something like that. Of course, that’s true for a lot of drugs, but I’m just pointing that out.
So if you’re interested in LDN, keep in mind it has to be prescribed by a physician, or in some states, a naturopath can prescribe it. You can print out some studies from PubMed. You can go into PubMed.org and search for “low-dose naltrexone,” and there are a bunch of studies that will pop out. You can print those out and take them to your doctor to discuss. There’s a website called LDNinfo.org that has kind of a clearinghouse of information on LDN that you can go to. There’s a Yahoo group about LDN that you can join and talk to folks there and try to find a practitioner in your area.
What I don’t recommend is ordering it from overseas pharmacies. You never know what you’re getting that way, and there have been a lot of studies showing that drugs that come from those pharmacies are not often what they claim to be, and that’s just flat out dangerous and not very smart. Hopefully that goes without saying, but I’m just mentioning it anyway.
And particularly with LDN, it should be obtained from a reputable compounding pharmacy that has some experience in compounding LDN. I mean, there are certain pharmacies that know which binders and fillers make the most sense with it and seem to be the best tolerated, and they just a lot more experience working with patients that are taking it, and it’s a good idea to refer your physician to one of those. Skip’s Pharmacy in Florida is the one that comes to mind that’s been doing it for the longest period of time, so you can look them up on the web. There’s also a list of recommended pharmacies on the LDNinfo.org site that you can make your doctor aware of.
Let’s see. Anything else come to mind? What have you got, Steve?
Steve Wright: I got a question. Have you seen in your patient population that, for instance, say someone settles on 3 mg, do they ever need to change that? Does the effect wear down over time, or do life circumstances sometimes mean that you could get more sensitive or less sensitive to it?
Chris Kresser: Great question. My sort of take is usually, like, let’s use any treatment, whether it’s a supplement or medication for a therapeutic purpose, to reach a therapeutic goal, and once we reach that goal, I’m always interested in seeing if we get people off of stuff, maybe once the immune system comes back into balance and the patient is symptom free. Like we’ve talked about before, the concept of tolerance. You’re an engineer, Steve. You’ve told me about it. It’s easier to maintain something within tolerance, that’s already where it should be, than it is to get it back there in the first place. A patient may want to stop taking LDN or titrate off of it after a while to just test to see if they can maintain the improvement that they’ve gained from it.
On the other hand, if somebody has a condition like Graves’ disease where there’s a real risk of going into a hyperthyroid storm and stroking out and that’s been historically an issue for them and LDN is just completely managing it without any other medication, if you’re going to weigh that against taking PTU or methimazole or pretty toxic medications that often needed for Graves’ or even more invasive, like a surgery to remove the thyroid or to radioactively ablate the thyroid gland, and you’re weighing those against just staying on LDN, of course, you have to talk to your doctor about these questions, but my take on that would be if it were me as a patient, I would rather take LDN on an ongoing basis than to face any of those outcomes. So it just depends on the person.
And the dose can fluctuate, depending, of course, on the background level of immune dysregulation. If maybe someone is gluten intolerant and they don’t know it and they’re eating gluten and they’re taking LDN and they need the full 4.5 mg dose because they kind of have their foot on the accelerator and the brake at the same time, but then they take gluten out of their diet and maybe 4.5 mg is unnecessary or even starts causing some side effects, so that’s possible.
Steve Wright: One more question.
Chris Kresser: Yeah.
Steve Wright: In previous shows and potentially in writing — I’m not sure where I remember you mentioning this — but you’ve said to commit to a timeframe for LDN because not everybody shows symptom reduction or lab test reduction at a specific point in time after starting taking it, so what are your current thoughts on that?
Chris Kresser: Yeah, it’s the same. I mean, it’s really interesting. Some people, like, the next day after they start they feel like a different person, and then other people, it can take three months for them to really feel a significant difference. We don’t really understand why that is yet. And interestingly enough, it doesn’t necessarily correspond to how sick they are or how long they’ve been sick. I’ve seen it where people have been really kind of in bad shape and they respond immediately and other people whose condition was a lot more benign or mild and they didn’t have an immediate response. I don’t know about that, but I do know that it’s common. So I would say probably give it three months before you let it go if you’re going to try it.
A couple other things to consider are that because LDN blocks the opioid receptors, some pain narcotic drugs like Percocet or morphine or tramadol, LDN can decrease their effectiveness so that typically they shouldn’t be taken together. And patients with Graves’ or Hashimoto’s that are taking thyroid meds should be careful because one thing we’ve seen happen is if someone takes LDN and their thyroid function improves, then the dose of medication they were on that was maintaining equilibrium before all of a sudden becomes too high, and that person can go into kind of like a hyperthyroid episode or start feeling heat or not sleeping well or all those typical symptoms. Your doctor should mention this to you when they prescribe it, but that’s something to be aware of and to talk about with your doctor if you’re on a thyroid medication, to be ready to reduce the dose if your thyroid function starts to improve.
A question that often comes up is, OK, are there some natural alternatives to LDN that achieve the same purpose of reducing central nervous system inflammation and promoting T regulatory cell function? Definitely, there are things that achieve both of those goals. In some cases, especially when you put them together, they can do just as good of a job as LDN, but in other cases I’ve seen LDN just be more effective even when someone’s done all these other things. But for Treg cell function, vitamin D is a powerful T regulatory cell promoter, as is glutathione, so those should definitely be in the repertoire. Maintaining adequate levels of selenium and zinc and iodine is important for immune function. Probiotics, especially bacillus species like soil-based organisms, promote Treg cell function. Butyrate, which is a short-chain fatty acid that’s produced by beneficial bacteria in the colon, improves Treg cell function, so prebiotics can actually do that indirectly. Vitamin A is important for immune balance, so cod liver oil. And then for inflammation, we have things like curcumin and boswellia — those are COX inhibitors, selective kinase response modulators, fish oil or EPA and DHA from cold-water fish, of course, and then diet obviously. Whether we’re talking about just a general, overall anti-inflammatory paleo-ish type of diet or whether you’re taking the next step and doing an autoimmune protocol type of diet, those can be important as well.
Steve Wright: Awesome. Well, it sounds like a pretty good round-out there. It seems like if people wanted to try those things, I’ve seen a lot of people try those things and not get success and then get on LDN and through LDN and some of those supplements together, like, really have a brand-new life.
Chris Kresser: Yeah, it can be pretty dramatic. And of course, I don’t want to create any false hope or unrealistic expectations for people, but for some it has definitely been life changing. I have patients who had been on those thyrotoxic drugs for 20 years or more, 25 years. One patient comes to mind who had Graves’ and had been on PTU for 20 years and was able to get off PTU completely and all other medications and just take LDN and feel better than she ever had felt during that period and maintain completely normal thyroid numbers, so it can be pretty dramatic. I have to say, though, that we have had patients who have taken it and experienced nothing at all. So it’s not a miracle, of course. No treatment is, but it helps a lot of people, and it does it pretty affordably and without causing a lot of side effects or complications or risks, and that’s a pretty good combination.
Steve Wright: Yeah, definitely. Awesome.
Chris Kresser: All right.
Steve Wright: Well, if listeners would like their question answered, make sure to go to ChrisKresser.com/PodcastQuestion to submit your questions. Chris and his team are always taking those in and trying to pull the most relevant topics that haven’t already been covered, so if you have submitted questions and you’re wondering, why, guys, haven’t we talked about my question, make sure you listen to the rest of our episodes because there’s quite a treasure trove of information that we’ve covered over, what, like, four or five years now?
Chris Kresser: Yeah, four or five years, somewhere in there. I should know, but something like that. Yeah.
Steve Wright: Awesome. And in between episodes, if you’re not following Chris on social media, this is where you can get updates on the latest articles he’s reading, different things that he’s pulled from around the web, so go to Facebook.com/ChrisKresserLAc and Twitter.com/ChrisKresser. Thanks for listening.
Chris Kresser: All right. Thanks, everyone. Talk to you next time.
pimg class=”alignright size-medium wp-image-54969″ src=”http://cdn.marksdailyapple.com/wordpress/wp-content/uploads/2015/04/primal_flora_30_400px-300×300.png” alt=”” width=”320″ height=”320″ /Anytime I a title=”Grok Didn’t Take Supplements So Why Should I?” href=”http://www.marksdailyapple.com/definitive-guide-to-primal-supplementation/”discuss supplements/a, some readers balk. For them, if a title=”What Would Grok Do?” href=”http://www.marksdailyapple.com/what-would-grok-do/”Grok didn#8217;t do it/a, we shouldn#8217;t either. And you know what? If that describes you, I get where you#8217;re coming from. Ideally, optimal health develops organically — from the food we eat, the sun, sleep, and movement patterns we follow, the lifestyles we develop. But we don#8217;t live in Grok#8217;s world any more. We don#8217;t have access to the a title=”What Did Our Ancient Ancestors Actually Eat?” href=”http://www.marksdailyapple.com/what-did-our-ancient-ancestors-actually-eat/”same nutrient-dense plants/a and animals he did, and we face entirely new stressors and endure novel deficits previous generations never have. These new challenges call for new solutions, and a title=”Managing Your Mitochondria: Nutrients and Supplements” href=”http://www.marksdailyapple.com/managing-your-mitochondria-nutrients-and-supplements/”supplements/a can be one of these solutions. As a supplement maker, I always take cues from a title=”What […]
In February this year, Beyoncé partnered with her trainer, Marco Borges, to create an organic, vegan, gluten-free, soy-free meal delivery service called 22 Days Nutrition. Beyoncé and Jay-Z went vegan for 22 days in December of 2013 with the help of Borges and both became enthusiastic supporters of the challenge. Thus, she went into business with her trainer to help other people feel as magical as she does. Sounds great, right?
Well, if it’s good enough for Bey, it’s good enough for me. Would I become closer to her if I tried the meal plan? Would I truly feel flawless? I decided to give her vegan meal plan a shot for 48 hours. Here’s how it went.
pimg class=”alignright size-full wp-image-54973″ src=”http://cdn.marksdailyapple.com/wordpress/wp-content/uploads/2015/04/passport.jpg” alt=”” width=”320″ height=”213″ /When I look back on my life and take stock of the things that have made and make me happiest, I don#8217;t think about the material objects I#8217;ve procured. I don#8217;t think about the money I#8217;ve made or the cars I#8217;ve owned or the possessions stashed away in my garage. I think about the experiences./p
pThere are the grand adventures: I did Outward Bound when I was 17. It was 28 days of rigorous experiences in the wild of New England — moment to moment instances where I had to #8220;be here now or maybe die#8221; — that majorly shaped the rest of my life, and for which I will be ever grateful. A journey to Europe alone at 22 with a backpack, a Eurail pass, and no agenda or itinerary (before the days of smartphones and apps and online reviews that eliminate […]
Microwaves. These handy gadgets have been the source of much debate in the online health community, and it’s not hard to see why. The idea of “zapping,” “nuking,” or otherwise heating your food using microwave radiation can seem a little dubious.
In this article, I’ll take a look at the evidence behind some of the most common microwave concerns. Do microwaves leak radiation? Do microwaves destroy the nutrients in food? Do they denature proteins and make food toxic to our bodies? First, though, let’s start with the basics. How do they work?
How do microwave ovens work?
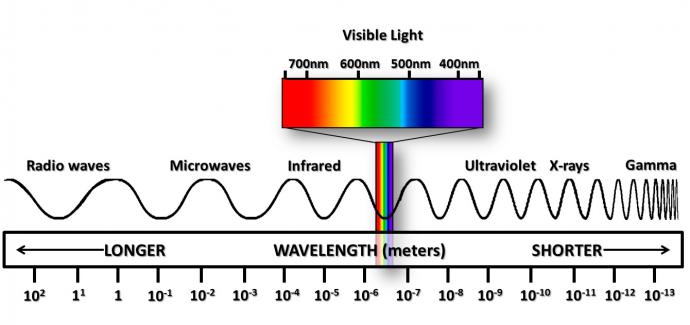
The aptly-named microwave oven uses microwave radiation to heat food. Electromagnetic (EM) radiation exists over a range of wavelengths, where shorter wavelengths (such as x-rays and gamma rays) have higher energy than longer wavelengths (such as radio waves). On the EM spectrum (pictured below), microwaves fall between radio and infrared waves.
Each level of radiation has different effects on the molecules they interact with. Microwaves contain enough energy to induce molecular rotation, which is the lowest energy form of interaction, but they don’t have enough energy to induce molecular vibrations, electron excitation, or ionization. Microwaves have the greatest effect on water molecules, due to their polar structure, and these rapidly rotating water molecules transfer energy as heat to the other molecules in food.
Do microwaves leak radiation?
One concern many people have about microwave ovens is the simple fact that they emit, well, microwaves. Hasn’t exposure to microwave radiation been linked to cancer and infertility? Evidence is mixed; most published research concludes that low-level microwave exposure doesn’t present a significant risk to human health. (1, 2, 3) Even if it did, this is only an issue if the microwaves inside the microwave somehow escape the microwave and encounter your body, which (as you’ll see below) is unlikely.
The FDA requires that microwaves emit no more than 5 mW/cm2 of radiation at a distance of 2 inches from the microwave. They also point out that microwave radiation dissipates rapidly as you move away from the source, so a measurement taken 20 inches from the microwave would be about 1/100 of the measurement taken at 2 inches. This is good news, because it means that to avoid radiation from your microwave, all you have to do is step away from it while your food is heating.
Are #microwaves as unhealthy as we are told?
The other good news is that in general, real microwave emissions seem to stay below the federally mandated maximum. A study published in 2013 on microwaves in Palestine found that the radiation leakage measured one meter from the microwave varied from 0.43 to 16.4 μW/cm2, with an average of 3.64 μW/cm2. (4) A 2001 survey of microwaves in Saudi Arabia concluded that with 95% probability, a microwave will be found to leak between 0.01 and 2.44 mW/cm2 at a distance of 5cm, and only one out of 106 microwaves surveyed was found to leak more than the FDA limit. (5)
For comparison’s sake, a 2013 study measured microwave radiation emitted by cell phones at a distance of 3.5cm from the phone, and found levels of 10 – 40 μW/cm2 during a call and 0.35 – 10.5 μW/cm2 on silent. (6) Based on these numbers, having a cell phone in your pocket on silent mode exposes you to roughly the same level of microwave radiation as standing one meter from your microwave while it’s heating food.
Honestly, just don’t press your face up against the door of the microwave while your food is cooking, and step a few feet away if you can. If you’re going to be concerned about exposure to microwave radiation, you’d probably be better off getting rid of your cellphone than your microwave oven. (But that’s a topic for a another day.)
Do microwaves make proteins toxic?
Now, let’s talk about the effect of microwave heating on food. One oft-cited claim is that microwaves can “denature” proteins, making them toxic to the human body. First of all, I think there are some misconceptions about what exactly “denaturation” is. Contrary to how the word is often used, it doesn’t mean that a protein has ‘changed’ in some unspecified way to make it more toxic. When a protein is “denatured,” that specifically means it has unfolded and lost its three-dimensional shape, but all of the amino acids in the protein are still bonded together.
Heat in general denatures proteins, so cooking your food (using any heating method) will denature the proteins. Cooking can even be defined as heating something enough to denature the proteins. (7) Changes in pH also denature proteins. In fact, guess what one of the functions of stomach acid is? Denaturing the proteins you ingest! Proteins need to be unfolded (denatured) before digestive enzymes can cleave them into individual amino acids to be absorbed in your small intestine. “Denatured proteins” don’t sound so scary any more, do they?
Perhaps what people have in mind when they refer to “protein denaturation” is actually isomerization of amino acids. This is a completely different process, but it is a change that actually affects the nutritive value of proteins. Without getting too into the chemistry, amino acids can exist in two configurations, termed D- and L-, and isomerization is the process by which an amino acid switches from one configuration to the other. Our bodies almost exclusively use the L- form of amino acids, but pH changes and heat can cause amino acids in food to isomerize to the D- forms, which can’t be efficiently digested or utilized by our body. (8)
A few studies where large amounts of isolated D- amino acids are fed to rodents show potential harmful effects, but there’s no evidence that the levels of D- amino acids normally found in food are harmful. (9) Plus, many foods (such as raw dairy from ruminants and some fruits and vegetables) naturally contain low levels of D- amino acids.
In any case, there doesn’t appear to be a significant difference in levels of D- amino acids in foods cooked in the microwave compared with foods heated conventionally. One study conducted in 1989 found higher levels of D- amino acids in microwaved formula compared with other heating methods (10), but several more recent studies have found no difference. (11, 12, 13, 14, 15) Additionally, the general consensus seems to be that if more D- amino acids are formed, it is due primarily to over heating or uneven temperature distribution, rather than a specific effect of microwaves themselves.
Do microwaves destroy nutrients?
As far as vitamins, minerals, antioxidants, and plant phenols, retention does not appear to depend on cooking method. Levels of nutrient retention were sometimes higher in microwaved food, and sometimes lower, depending on time, temperature, and amount of water used in the cooking process. (16, 17, 18, 19, 20)
In general, nutrients are lost from food during any type of cooking, and more nutrients are lost when the temperature is higher or the food is cooked for longer. Water soluble vitamins are readily leached into cooking liquid (no surprise there), so boiling food tends to result in greater nutrient losses than microwaving it with a small amount of water (unless you drink the water you boiled the food in, in which case you’d still be getting most of the nutrients).
As a final interesting data point, one study published in 1995 used a rat model to look at the overall effects of a microwaved diet in vivo. The diet consisted of meat, potatoes, vegetables, and some oil, cooked either in the microwave or conventionally, and was fed to rats for 13 weeks. To magnify any adverse effects of microwave cooking, the study authors added two additional experimental groups that received “abused” food, which had been reheated and cooled a couple times either conventionally or in the microwave. (21) At the end of 13 weeks, they found no adverse effects of microwave cooking on the rats.
Don’t fear the microwave!
In conclusion, microwaves aren’t as scary as some people make them out to be. Yes, they’re another source of microwave radiation in your home, but the levels are extremely low, and can be almost entirely avoided by simply stepping away while your food is heating. And compared with microwave radiation from other devices (particularly cell phones), radiation from your microwave oven is negligible.
Additionally, there’s no evidence that microwaves adversely affect the nutrient profile of foods. Because microwaves are a relatively new device, I prefer to think of them as “guilty until proven innocent” rather than the other way around, but given what we know about EM radiation and its effects on food molecules, there isn’t really a mechanism by which microwaves could destroy nutrients other than heat. And heat, of course, is an issue regardless of cooking method!
If you’re still skeptical of microwaves after reading this, by all means – use whatever cooking method makes you comfortable. I might be one of the few freaks in the world now that still doesn’t use a microwave, but I can’t say that it’s because of any safety concern or scientific concern. I’ve just never liked what they do to the texture of certain foods, and for whatever reason, I’ve never gotten into using one.
But if you enjoy the convenience of a microwave, don’t be afraid to use it – especially if being able to microwave your food makes the difference between heating up leftover Paleo chili or grabbing a Nutri-Grain bar for lunch!
What do you think about microwaves? Did reading this article change your opinion of them? Let me know in the comments!
pimg class=”alignright size-full wp-image-54953″ src=”http://cdn.marksdailyapple.com/wordpress/wp-content/uploads/2015/04/moon2.jpg” alt=”” width=”320″ height=”213″ /For today#8217;s edition of a title=”Dear Mark” href=”http://www.marksdailyapple.com/category/dear-mark/”Dear Mark/a, we#8217;ve got three questions and three answers. First, the full moon sure is pretty and big and bright at night, but can it produce (or reflect, rather) enough a title=”How Light Affects Our Sleep” href=”http://www.marksdailyapple.com/how-light-affects-our-sleep/”light to disrupt our melatonin production/a? Should we be blocking out moonlight, too? Next, do exercise non-responders exist? If not, what else can explain the curious case of a lifelong heavy lifter who has nothing – physique-wise – to show for it? And finally, a recent article in Slate makes the claim that weight loss is basically impossible and not even all that good for you. Is the author right? Is the author wrong? See my thoughts on the matter down below./p
pLet#8217;s go:/p
pspan id=”more-54947″/span/p
blockquotepHi Mark,/p
pCompletely blacking out a room for sleep seems to be all the rage these days, […]
For now classes are 6pm and 640pm at 2840 Wildwood st in the Boise Cloggers studio.
Book your class NOW!
click this ==>
Warrior Fit Testimonials
First, I want to say thank you for convincing me to do Tabata! I was struggling to lose weight and Finally I found something that helped! I really appreciate your coaching! - Craig T.
Ever since I was convinced to do Tabata I have seen huge results, I lost 6 pounds and gained energy in the first 3 weeks. I have been working out for 3 months before I decided to do Tabata and I struggled to lose weight.
At first I thought "How am I losing weight by bringing my heart rate up then cooling down then bringing it up again?" I don’t know how it works but it does!
Thank you!! - Theresa F.
The first day of Tabata, I wondered WHAT AM I DOING - I AM 56 !! Five weeks later I knew that it was what I needed. I learned that I could push myself well beyond my comfort zone and feel good later. I have a marked improvement in physical as well as emotional endurance. - Lyn C.
When I was first told about Tabata I was very excited from the word go, however that excitement stemmed from the fact that I had no clue what it meant. I missed the first week of class b/c I was traveling for work so when I came in during the 2nd week I had some making it up to do.
It was hard at first b/c my body wasn't used to working out at such a fast pace, but once I got into a rhythm I started to feel very good. These classes are no joke. If you stick with it you will leave there feeling stronger, healthier and overall better about yourself and what you've accomplished.
I would recommend these classes to anyone. Darrin is a great trainer and he'll keep you going with his energy.
- Jami L.
Warriors Fit Audio
Warrior Fit uses High Intensity Music to get ya Moooovin' So we can all "Get Our Sweat On"
The link below will give ya a freeee shot at Audible plus a couple audio books just to try it out and if you haven't used audio books on your commutes you are missing out. Get pumped up before you get to where you are going and exercise your mind. I use it Everyday. Go get yours now!







 This
This 

 This
This 
 For now classes are 6pm and 640pm at 2840 Wildwood st in the Boise Cloggers studio.
Book your class NOW!
click this ==>
For now classes are 6pm and 640pm at 2840 Wildwood st in the Boise Cloggers studio.
Book your class NOW!
click this ==>








{kind=link}
{kind=link}